

#apaperaday: Variants in the Sequence of the Probe Hybridization Site May Affect MLPA Performance in Patients with Duchenne/Becker Muscular Dystrophy
In today’s #apaperaday, Prof. Aartsma-Rus reads and comments on the paper titled: Variants in the Sequence of the Probe Hybridization Site May Affect MLPA Performance in Patients with Duchenne/Becker Muscular Dystrophy
From the journal of applied laboratory medicine by Buitrago et al on the multiplex ligation dependent probe amplification (MLPA) in Duchenne and the risk of false positive if there is a small mutation under the probe DOI: 10.1093/jalm/jfac136
I commend the authors for publishing so clearly about this topic as many people who should be aware of the risk for false positives are not. Some context: Duchenne and Becker muscular dystrophy are caused by mutations in the dystrophin gene. Deletions of one or more exons occur in ~65% and duplications of one or more exons in ~10% of patients. ~25% of patients has a small mutation within an exon or one that disrupts splicing.
As 75% of dystrophinopathy patients has a copy number variation in exons (deletion or duplication), looking first for these mutations is most cost effective. The MLPA analysis does this: For each exon there is a pair of probes that are ligated only if the probes bind.
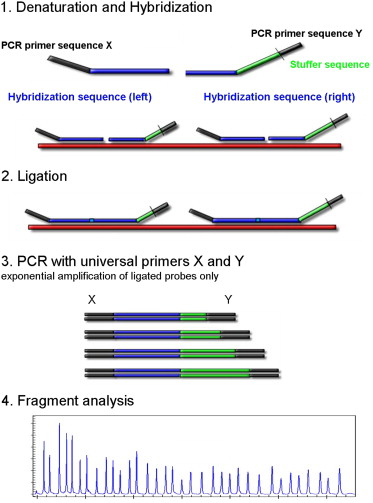
Then a PCR is done with primers targeting the outer regions of the ligated probes. Only ligated probes will be amplified. When there is a deletion, the probes are not ligated, so no amplification. When there is a duplication, more probes are ligated, so more product is amplified.
Each ligated probe has a specific length so after amplification a fragment run is done, where you know that the length of the ligated probe for exon 1 is a certain length, the one for exon 2 is a certain length etc. Missing probes: deletion. Extra high peak: duplication.
Now to the problem of false positives: then an exon has a small variant (pathogenic or not) within an exon, that can prevent the binding of one of the two probes. Then there is no ligation possible, and therefore no amplification. One the fragment run this shows as a deletion. However, the exon is actually there! For this reason it is crucial for single exon deletions to do an extra test to see whether 1. the exon really is deleted 2. the exon is actually there but harbors a variant (pathogenic or not).
In this study authors wanted to test how big of a problem this actually is. They had a cohort of 111 males from Colombia suspected to have Duchenne or Becker. For 72 they found a deletion or duplication by MLPA. 62 had deletions of multiple exons or duplications. 10 patients had a single exon deletion. Authors did the mandatory secondary analysis: 4/10 patients did not have a deletion, but a variant within the exon! Authors stress that this underlines how important it is to do the second analysis for single exon deletions deteced by MLPA
Knowing the right mutation is crucial, as it allows prognosis (Duchenne or Becker), genetic counseling and disease management, which for some mutations means mutation specific therapies.
To underline how things can go wrong: a deletion of exon 50 would be eligible for exon 51 skipping. However, if that deletion is a false positive for a nonsense mutation within exon 50, the patient actually is eligible for stop codon readthrough therapy!
So the take home message is: make sure you confirm single exon deletions detected by MLPA are really deletions & not small mutations in the dystrophin gene. If you see a single exon deletion in a diagnostic report, check whether this second analysis was done as per the guidelines.

